Grappling with the Grief Clinicians Carry
Reflection on Training
We came to a January training to teach legacy-building for families through experiential learning. We left with a deeper truth: clinicians need, and deserve, a space to process their own grief and loss together. At this recent training, we set out to teach legacy-building for families through experiential learning. What emerged was something deeper: clinicians sharing their own experiences of loss and creating space to process grief together,
During a recent Compassionate End-of-Life training with pediatric oncology providers in Eldoret, Kenya, we intentionally incorporated memory-making activities — tools designed to help families honour the life of a child facing cancer. We invited participants to reflect on how these tools might support families through death and bereavement. As the conversation unfolded, clinicians began sharing their own experiences of loss. One reflected, “Death is an eventuality, but without appropriate skills, handling it becomes a burden — and that’s why most healthcare providers are evasive in talking and supporting others or themselves.” Another participant said, “This training doesn’t just change how you work — it changes how you are at work.”
As a group, we realised how rarely clinicians are given permission, space and time to acknowledge the grief they carry. Paediatric healthcare workers regularly accompany families through the death of a child - yet their own grief often remains unspoken and unprocessed.
The Grief We Don’t Name
Across cultures and health systems, how we process grief related to loss is complicated. When a loved one dies of an extended illness or a relative is in a traumatic accident, we all grieve. In healthcare, we are often faced with work-related loss and death of our patients as well.
This essential work raises profound and often unspoken questions:
How do you make space for existing grief?
What do providers need to process?
How can we, even as well-meaning professionals, underestimate this need?
Often, grief goes unnamed because competence is valued more visibly than vulnerability. We teach communication frameworks, symptom management and ethical decision-making. Processing grief - both personal and professional - is foundational to sustaining compassionate care. With busy clinical schedules, it’s hard to find structured space for clinicians to process the emotional weight of repeated child deaths. We rarely build in time for reflection on the children whose names still surface unexpectedly. This is where acknowledging grief becomes essential, especially in caring for children with serious illnesses.
When Grief Is Unacknowledged— and When It Is Integrated
Unacknowledged grief carried by healthcare workers can quietly, yet profoundly, manifest in care:
Emotional numbing
Avoidance of difficult conversations
Over-identification with certain families
Compassion fatigue
Moral distress
But when grief is acknowledged and integrated, it can lead to:
Deeper presence
Authentic empathy
Boundaried compassion
Sustainable practice
As one participant reflected, “The training helps you look inward before you are empowered to outwardly hold space for others.”
Using Legacy Work to Process Personal Grief
The training was led by Global Treehouse and AMPATH, with on-site faculty including Elizabeth Kabuthi, Erin Das, Dr Esther Wanjama and Pamela Were. During the training, we collectively facilitated several legacy activities that the team at Moi Teaching and Referral Hospital (MTRH) often used in paediatric settings to support families in making meaning and creating legacy items with their children. We asked participants to participate in the activities on a personal level, thinking and reflecting on a personal loss that they have experienced. This is part of a large project to impact bereavement support across the country, including with peer groups.
Research in paediatric palliative care has demonstrated the importance of legacy-building for children and families facing life-limiting illness. The work of Lori Wiener and colleagues (Wiener et al., 2018) highlights how legacy activities help create meaning, preserve identity and support continuing bonds after a child’s death. Studies examining moral distress in end-of-life care environments, including work by Sarah McArthur and colleagues (McArthur et al., 2016), show how clinicians absorb the emotional and ethical weight of serious illness care. Without intentional opportunities to process these experiences, that weight can accumulate.
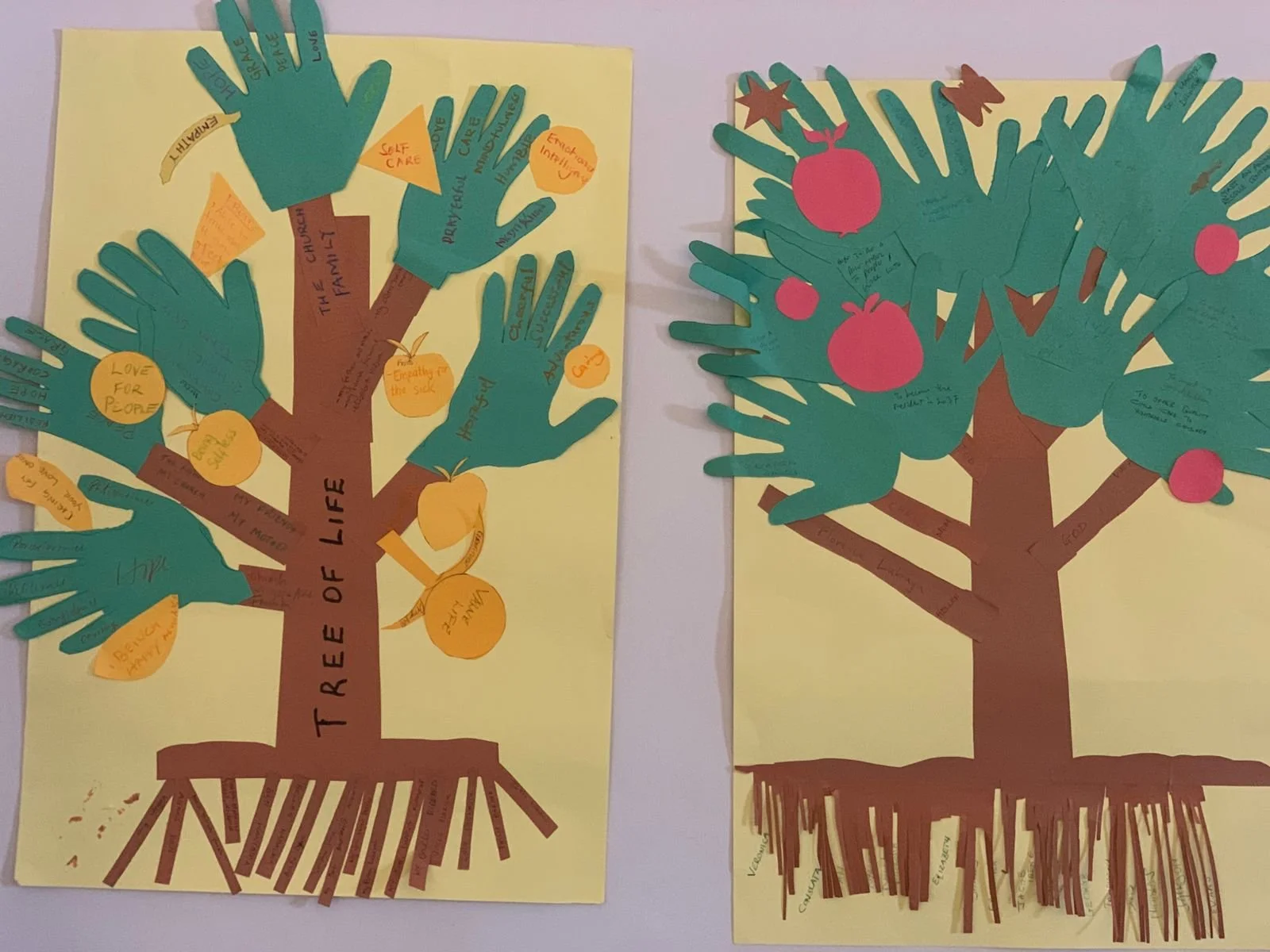
In the Tree of Life exercise, participants wrote the name of someone important who had died in the roots of the tree, symbolising the foundations that continue to shape their lives. They then traced their hands as leaves, writing hopes for the future connected to that person’s legacy. In the Memory Collage activity, providers created scrapbook pages honouring someone they had lost, including favourite memories or a picture of something that they did together.
These exercises were designed to help them process their own grief as well as model tools clinicians could use with families. Legacy-making allowed clinicians to externalise memory, speak names aloud and reflect in the safe community of colleagues. This activity offered a structured way to acknowledge continuing bonds — not only for patients and families, but for providers themselves. When clinicians are permitted to grieve and hard conversations become less avoidant. One participant described the experience as “a learning, relearning, and unlearning training combined with a therapy session.”
“We may consider asking ourselves, what is the relationship between tending our own grief and supporting others through theirs? It is the difference between performing empathy and embodying it.”
Being Present in the Face of Loss
If paediatric oncology and palliative care inherently involve loss, then making space for grief must be embedded into our professional development — not treated as an afterthought. This can include:
Integrating reflective and legacy-building exercises into training curricula
Normalising debriefs after the death of a child
Creating rituals that honour both families and staff
Teaching leaders to recognise cumulative grief in their teams
Acknowledging personal loss and grief can be sparked in a professional setting as clinicians support families and children through a difficult illness
During the two days, we were reminded how important it is to slow down and make space for grief — even when clinical schedules are busy. When clinicians are given space to process their own losses — and to slow down and make space for that grief, even amidst busy schedules — they can be more fully present and offer truly sustainable compassion to the families they serve.
References
The need for grief support in paediatric serious illness care is supported by both research and global policy guidance, including the following foundational works:
Ferrell, B. R., Coyle, N., & Paice, J. A. (2015). Oxford textbook of palliative nursing (4th ed.). Oxford University Press.
McArthur, S., Broom, A., Kirby, E., Good, P., Wootton, J., & Adams, J. (2016). Negotiating moral distress in end-of-life care: A qualitative study of clinicians. Social Science & Medicine, 164, 25–33. https://doi.org/10.1016/j.socscimed.2016.07.028
Wiener, L., Rosenberg, A. R., Lichtenthal, W. G., & Weaver, M. S. (2018). Legacy building in pediatric palliative care. Journal of Pain and Symptom Management, 55(2), 535–544. https://doi.org/10.1016/j.jpainsymman.2017.09.020
World Health Organization. (2018). Integrating palliative care and symptom relief into pediatric oncology: A WHO guide for planners, implementers and managers. World Health Organization.